
Authors: N.V. Skrypnyk, MD, PhD, Professor, T.S. Vatseba, PhD. SHEI Ivano-Frankivsk National Medical University, Department of Endocrinology
The relevance of the problem. The metabolic syndrome (MS) is a multifactorial clinical condition caused by a complex of genetic, hemodynamic, neurohumoral features and lifestyle. The medical and social significance of MS lies in the high mortality rate from its consequences. For example, in people with MS, mortality from coronary heart disease (CHD) increases by 40%, from arterial hypertension (AH) – by 2.5-3 times, and from type 2 diabetes mellitus (DM) – by 4 times. The importance of studying MS also lies in its high prevalence. It affects 14 to 24% of the population in economically developed countries. The prevalence of MS among the adult population is quite high and, for example, in the United States is 23.7% (24% among men and 23.4% among women). According to the WHO, in 1999, the incidence of MS among men was 27%, and among women – 19.7%. In 2001. NCEP ATPIII (The third report of the National Cholesterol Education Program expert panel on detection, evaluation, and treatment of high blood cholesterol in adults – Adult Treatment Panel III) determined the incidence of MS among men to be 25.9%, among women – 23.4%, and in 2004 – 32.2 and 28.5%, respectively. Unfortunately, there is no systematized data on the prevalence of MetS in Ukraine. The list of metabolic disorders included in the concept of MS has been constantly changing over the past 15-20 years. The presence of a single pathogenetic mechanism allowed G. Reaven in 1988 to identify MetS as an association of abdominal obesity, impaired glucose tolerance or type 2 diabetes, dyslipidemia, and hypertension. The current identification of MetS is carried out in accordance with the 1998 WHO guidelines, the recommendations of the Third Report of the Expert Panel on the Detection, Evaluation and Treatment of Hypercholesterolemia within the framework of the US national educational program, the International Diabetes Federation (IDF).
In 2005, the IDF presented its new definition of MetS. The criteria for MetS recommended by the IDF are: the presence of visceral obesity as measured by waist circumference (WC (cm)), taking into account the specifics for different ethnic groups (Europeans: >94 cm in men, >80 cm in women) plus the presence of any two of the four factors listed: elevated triglycerides (TG) >1.7 mmol/L or specific lipid-lowering therapy; lowered high-density lipoprotein (HDL) <1.03 mmol/L in men and <1.29 mmol/L in women or specific therapy for dyslipidemia; hypertension (systolic blood pressure >130 mm Hg or diastolic blood pressure >85 mm Hg) or antihypertensive therapy for previously diagnosed hypertension; elevated fasting plasma glucose >5.6 mmol/L or previously diagnosed type 2 diabetes.
The clinic of MetS is determined by its main manifestations – obesity, hypertension, dyslipidemia, insulin resistance (IR) and diseases associated with it: heart and vascular disease, polycystic ovary disease, sleep apnea, gout, non-alcoholic fatty liver disease (NAFLD), and some forms of cancer.
MS is not considered a separate diagnosis or nosological form, but it is important for the prognosis and treatment of the underlying disease. The main unifying factor of metabolic disorders is IR. Decreased insulin sensitivity causes compensatory hyperinsulinemia, so the latter is often used as a marker of insulin resistance in clinical and epidemiological studies. R. De Fronzo compared this condition to an iceberg: on its surface there are clinical manifestations (DM, CHD, hypertension, obesity), which usually come to the attention of doctors, and at the core there is a complex of metabolic disorders caused by IR.
Over the past decades, the international community has been paying special attention to overcoming the consequences of iodine deficiency (ID) on a global scale, considering it as a solution to one of the global health problems.
After the Chornobyl accident in 1986, thyroid pathology ranked first among all endocrinopathies in Ukraine.
Almost the entire territory of Ukraine is in the zone of ID of varying severity. Prevention of iodine deficiency diseases (IDD) remains an acute problem. This is especially true in the Carpathian region, where there is a lack of iodine in soil, food and water.
Hypothyroidism is recognized as an important consequence of diabetes, which is considered by modern medical science to be one of the risk factors for cardiovascular disease. There is an increase in the incidence of hypothyroidism. The prevalence of thyroid hypofunction among women ranges from 4 to 21%, among men – 3-16%.
The literature data available today on the frequency, prevalence and functional status of the thyroid gland in patients with MS in different regions are few and rather contradictory. It should also be noted that the impact of impaired thyroid function on the realization of insulin function is currently studied in few experimental studies. The increase in the incidence of thyroid pathology, including hypothyroidism, in patients with MS is indicated by single studies, and it has also been noted that the incidence of hypothyroidism and nodular goiter in patients with MS significantly increases with age. The high prevalence of hypothyroidism in women with menopausal syndrome has been proven.
Recent studies have established the influence of thyroid hormones on insulin action and the relationship between thyroid function and IR, although these relationships are quite complex. How does hypothyroidism contribute to the development of IR? The answer to this question should be sought in the factors that form IR: visceral obesity, dyslipidemia, inflammation, oxidative stress, endothelial dysfunction, hypertension, activation of the sympathetic-adrenal and renin-angiotensin-aldosterone systems, genetic predisposition, and hemostatic disorders.
Metabolic disorders inherent in type 2 diabetes as part of MS, leading to discoordination of many organs and systems of the body, directly affect the functional state of the pituitary gland and thyroid gland. The analysis of well-known complications of the cardiovascular system demonstrates the possibility of developing hypothyroidism-induced IR syndrome in patients with MS. The prerequisites for this were obtained after the identification of a close pathogenetic relationship between the levels of hormones of the pituitary-thyroid system and the main components of this syndrome. Given the important role of thyroid hormones in ensuring the normal functioning of the cardiovascular, nervous and other body systems, as well as their effect on metabolism, which is already affected in diabetes, it is possible to assert the importance of the functional state of the thyroid gland for the course and prognosis of type 2 diabetes. Hypertension is often one of the first clinical manifestations of MS and hypothyroidism. The hypothyroid state leads to an increase in vascular resistance and vasoconstriction in the systemic and renal vessels, and the occurrence of hypertension. The most studied cardiovascular complications of hypothyroidism include dyslipidemia. Obesity is one of the most frequent and dangerous manifestations of thyroid hypofunction, and there is a close pathogenetic relationship between them. In recent years, the regulatory effect of thyroid hormones on the metabolism of adipose tissue hormones (leptin, adiponectin, resistin) has been revealed. The literature provides data on the presence of a significant imbalance in hormonal status in individuals with MS: decreased levels of thyroid-stimulating (TSH), somatotropic (TSH) hormones, triiodothyronine (T3), tetraiodothyronine (thyroxine, T4) and increased levels of adrenocorticotropic hormone, cortisol and aldosterone, as well as hyperandrogenism in women and relative hypogonadism in men. At the same time, the state of thyroid metabolism and structural changes in the thyroid gland in patients with MS have not been studied sufficiently. Hypothyroidism is associated with increased cardiovascular morbidity and mortality.
The main idea behind the concept of MS is to identify a population at high cardiovascular risk. Therefore, preventive measures to modify lifestyle and the use of adequate medications can significantly improve health indicators and prevent the onset and progression of both atherosclerotic vascular disease and type 2 diabetes, which, in turn, are inextricably linked to increased morbidity and mortality in the population. Thus, the need to improve the methods of diagnosis and treatment of patients with MS with type 2 diabetes is due to the fact that until recently, in the treatment of patients with this pathology, no due attention was paid to the functional state of the thyroid gland. In this regard, there is a problem of in-depth study of the therapeutic efficacy of new drugs – correctors of disorders of the metabolic link of homeostasis, IR, immune system, and functional state of the thyroid gland in the setting of ID.
Hypothyroidism and insulin resistance. Thyroid hormones play a significant role in metabolic and various processes. Most effects are mediated through mechanisms that stimulate the rate of metabolic processes, increase energy expenditure, and modulate the number of adrenergic receptors and thus sensitivity to catecholamines. Thyroid hormones affect the metabolism of carbohydrates in skeletal muscle and adipose tissue through positive transcriptional regulation of the muscle/fat-specific glucose transporter (GLUT 4), and stimulate lipolysis. All these effects interact with the action of insulin. It is known that insulin and insulin-like growth factor 1 are synergists of TSH in inducing thyroid tissue growth. It follows that hyperinsulinemia inherent in MS can contribute to the formation of a goiter even with normal or slightly elevated TSH levels. It should also be borne in mind that in the setting of ID, thyroid cells become particularly susceptible to TSH. In obesity, the conversion of thyroxine to biologically inactive reversible triiodothyronine in peripheral tissues increases, which can lead to peripheral hypothyroidism, which aggravates IR. An increase in the frequency of thyroid pathology, including hypothyroidism, in patients with MS is indicated by the studies of K.B.H. Lajimi, which revealed a negative correlation between elevated TG levels and thyroxine and a positive correlation with TSH. It has also been noted that the incidence of hypothyroidism and nodular goiter in patients with MS significantly increases with age. The high prevalence of hypothyroidism in women with menopausal syndrome was noted by N.V. Izmokerova. According to the authors, the algorithm for the examination of women with severe and/or prolonged menopausal syndrome in combination with atherogenic dyslipoproteidemia should include the determination of TSH.
Subclinical thyroid dysfunction is a biochemical concept. TSH level of 0.45-4.5 mIU/L in the absence of antithyroid antibodies is considered normal. In 2003, the American Association of Clinical Endocrinologists defined TSH levels (0.3-3.0 mIU/L) at which doctors can consider prescribing thyroid hormone treatment. The literature discusses TSH levels (2.5 mIU/L), which can be considered higher than normal. Among the clinical manifestations of subclinical hypothyroidism (SH), it is worth noting the manifestations of the cardiovascular system that threaten human life. In SG, there is an increase in blood pressure, especially diastolic blood pressure, and, as a result, an increase in total peripheral vascular resistance, an increase in the thickness of the carotid intima-media, impaired endothelium-dependent vasodilation with the development of endothelial dysfunction. HF is an undoubted risk factor for atherosclerosis. The severity of coronary atherosclerosis in patients with SH doubles, and this difference disappears with L-thyroxine replacement therapy. HH is associated with an increase in cardiovascular morbidity and mortality, which may be due to hypofibrinolytic and hypocoagulable states. The pronounced effect on the cardiovascular system in MG may be due to the fact that endothelial and smooth muscle cells have TSH receptors. The risk of cardiovascular disease increases significantly at TSH levels >2.5 mIU/L and is associated with an increase in low-density lipoprotein cholesterol (LDL-C), TG, myocardial dysfunction, and endothelial dysfunction. OH is considered a syndrome of chronic nonspecific inflammation. TSH induces the production of tumor necrosis factor-α (TNF-α) by bone marrow cells, increases the erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) and interleukin 6 (IL 6). It has been shown that in HH, an increase in ESR, CRP, and blood coagulation disorders is observed regardless of other factors (age, gender, cardiovascular disease, etc.) and regresses with the administration of thyroid hormones. There are reports of a relationship between IR and TSH levels in obese patients. Normal pituitary regulation maintains a model of thyroid function: low T4 associated with high TSH. However, in IR, negative associations between free thyroxine and TSH are developed, which contributes to peripheral resistance to thyroid hormones. Animal experiments have shown that a mutation in the α-isoform of the thyroid hormone receptor leads to thyroid hormone resistance, slowing of the heart rate, and IR. Deiodization plays an important role in maintaining circulation and thyroid hormone levels in tissues. T4 is converted to T3 via type 2 deiodinase in the brain, pineal gland, and muscles. A decrease in the activity of type 2 deiodinase can lead to a decrease in the intracellular concentration of thyroid hormones in these tissues. A decrease in intracellular T3 leads to an increase in TSH levels and a decrease in GLUT 4 transcription in insulin-sensitive tissues, such as skeletal muscle and adipose tissue, which cause IR.
Dyslipidemia in hypothyroidism. There are few studies investigating the effect of insulin on lipid metabolism in patients with hypothyroidism. The relationship between thyroid function and dyslipidemia has been proven. The reliable relationship between overt hypothyroidism and hypercholesterolemia has long been recognized, but there is little information about this relationship for the SG. It has been proven that the ratio between TSH and cholesterol is altered in patients with IR. Thus, individuals with elevated TSH and IR levels are more likely to develop dyslipidemia. Evidence suggests that TSH levels and tissue insulin sensitivity have important effects on blood lipids in type 2 diabetes. Decreased thyroid function is usually accompanied by impaired lipid metabolism, including increased levels of total cholesterol (TC), LDL-C, LDL-C, TG, and decreased HDL-C. These important factors further form the prerequisites for cardiovascular risks and encourage a deeper study of the mechanisms of hypothyroidism and understanding of its importance as a possible component of MS. The results of the studies indicate the mechanisms of dyslipidemia development in hypothyroidism, which are manifested by a decrease in the activity of cholesteryl ester transfer protein, which is a key factor in the metabolism of HDL and hepatic lipase (PL), which provide 30% of reverse transport of HDL; disruption of the structure of HDL and apo-A1 and apo-E (increase in phospholipids); decreased number and sensitivity of LDL receptors in the liver; impaired renal glomerular function (decreased glomerular filtration rate) and slower clearance of LDL, as well as decreased fat utilization and activation of TG mobilization from adipose tissue, impaired transport and excretion of atherogenic lipids in bile. In obese hypothyroid patients, free fatty acids (FFAs) are produced in excessive amounts, which are a transport form of fat transfer to body cells. The release of fatty acids is provided by the hydrolysis of TG. FFAs reduce the sensitivity of cells to insulin, lower the level of anti-atherogenic HDL, promote the formation of extremely atherogenic small dense LDL particles, increase plasma TG levels, have a toxic effect on pancreatic cells and have been shown to affect their apoptosis.
The accumulation of FFAs in the liver leads to excessive synthesis and release of glucose into the blood, promoting hyperglycemia and causing the effect of “glucolipotoxicity”, and also stimulates the development of peripheral and systemic hyperinsulinemia. Under conditions of dyslipidemia and IR, the physiological effect of insulin also changes, hyperinsulinemia becomes pathological and leads to the progression of atherosclerosis and coronary heart disease through a cascade of metabolic disorders.
Obesity, adipocytokines, and hypothyroidism. Visceral obesity is a manifestation of decreased thyroid function due to the lack of sufficient lipolytic action of thyroid hormones, slowing of basal metabolism, and decreased fat metabolism. Manifestation of obesity in hypothyroidism occurs due to slower dehydrogenation of fatty acids and reduced lipolytic activity of adipose tissue, reduced activity of catabolic processes, slower thermogenesis, and fluid retention in the body. In turn, obesity is the main component of the IR syndrome. It has been proven that adipose tissue contains receptors for thyroid hormones and TSH. Given the effect of thyroid hormones on adrenoceptors by potentiating the action of catecholamines that stimulate the action of the glucose transporter GLUT 4, it becomes clear that the stimulating effect of catecholamines on the receptor apparatus of insulin-sensitive target organs in hypothyroidism, which leads to IR, is reduced.
The latest research confirms that obesity is not equivalent to IR; obesity can modify insulin action, but not as a dominant factor, but as one of the causes. Data have been obtained indicating the existence of a relationship between TSH levels and body mass index (BMI) in non-obese patients.
The main role in the development of IR in obesity, which is very common in hypothyroidism, belongs to adipose tissue of the visceral region, which has a high metabolic activity, both lipogenesis and lipolysis processes occur in it. The function of adipose tissue, as well as the processes of lipolysis and lipogenesis, is influenced by catecholamines, corticosteroids, insulin, and the central nervous system. According to modern concepts, white adipose tissue is an endocrine organ, synthesizing more than 30 biologically active substances involved in the regulation of a wide variety of functions. In recent years, a number of authors have been studying the role of adiponectin, resistin, and leptin in the regulation of basal metabolism in patients with reduced thyroid function. At the same time, addressing the true role of adipocytokines in the formation of obesity-associated insulin resistance is a difficult task due to a number of contradictory data. The results of studies on the involvement of adipocytokines in pathogenetic processes, both in manifest and in the case of hypertension, do not provide an unambiguous answer. Recent studies have shown that in patients with hypothyroidism syndrome, the content of cytokines that cause impaired tissue microcirculation and hypoxia, which provokes the activation and accumulation of free radicals, heart damage, endothelial vascular dysfunction with subsequent increase in tissue hypoxia and impaired oxidative processes, increases significantly. Moreover, hormone replacement therapy does not always normalize cytokine levels.
Many of these substances have been shown to affect insulin sensitivity: leptin, adiponectin, TNF-α, IL 6, VLC, acetylation-stimulating protein, plasminogen activator inhibitor 1, transforming growth factor-β, angiotensinogen, etc. Adipocytes secrete large amounts of substances (cytokines), which are divided into proinflammatory (TNF, IL 6, CRP) and anti-inflammatory (adiponectin, leptin, resistin, etc.). Numerous studies have shown that obesity-related IR is associated with chronic inflammation and elevated levels of cytokines that can activate signal-operated cytokine suppressor proteins (SOCS) in tissues. As a result of increased adipokine activity, a chronic inflammatory process is induced, the main mediator of which is CRP, which is currently recognized as a marker of cardiovascular disease risk. CRP levels approaching the upper limit of normal are associated with MS. A prospective study by M. Christ-Crain et al. (2003) was the first to demonstrate an increase in blood CRP levels with the progression of thyroid insufficiency, allowing us to attribute elevated CRP levels to additional risk factors for cardiovascular disease in hypothyroidism.
Endothelial dysfunction and hypothyroidism. Thyroid hormones and TSH affect endothelial dysfunction, which is characterized by worsening of endothelium-dependent vasodilation in arterioles in patients with TSH levels above 4.1 mIU/L. Importantly, T4 hormone promotes skeletal muscle relaxation by counteracting arterioles. Thus, thyroid hormones behave as vasodilators, acting mainly on smooth muscle vessels. The hypothyroid state leads to an increase in vascular resistance and vasoconstriction in the systemic and renal vessels. As a result, studies suggest that thyroid function can cause dyslipidemia by altering insulin sensitivity in healthy individuals and patients with type 2 diabetes.
Microhemodynamics and hypothyroidism. An important component of glucose utilization is the effect of insulin on blood flow. Disruption of this mechanism in insulin-sensitive tissues can affect IR in obese patients with type 2 diabetes. In conditions of thyroid hormone deficiency, the physical properties of red blood cells deteriorate, which can cause impaired rheological properties of blood (with the appearance of sludge, microthrombi) and, as a result, extravascular changes – perivascular edema. The main pathological factor causing microhemodynamic disorders in some diseases is an increase in blood viscosity, which affects microhemocirculation, leading to blood resistance and increased blood pressure. Published data confirm that reduced blood flow in adipose tissue and muscles can be considered one of the pathogenetic mechanisms of IR in hypothyroidism. The main conclusion in explaining the majority of metabolic disorders in hypothyroidism is a decrease in blood flow in adipose tissue.
Hepatobiliary system in hypothyroidism. Thyroid hormones regulate the basal metabolism of all cells, including hepatocytes, which affects liver function, and the liver, in turn, metabolizes thyroid hormones, thereby regulating their systemic endocrine effects. The liver acts as the main organ that regulates the concentration of thyroid hormones in the blood by regulating the synthesis of thyroid hormone transport proteins, metabolizes thyroid hormones through oxidative deamination, deiodination, conjugation, and by regulating the processes of enteropathic circulation, as a result of which 80-90% of iodine contained in the body is reused and used in the re-biosynthesis of thyroid hormones.
Studies show that even with minimal thyroid insufficiency, there is an increase in the incidence of hypotonic biliary dyskinesia with cholestasis, and impaired fat breakdown and absorption, in turn, exacerbates atherogenic dyslipidemia, contributing to IR. Along with dysfunctional disorders of the biliary tract of the hypokinetic type, signs of impaired liver function are detected with an increase in the level of transaminases in some cases. Decreased thyroid function can directly affect the structure and function of the liver. In this case, there are two types of liver pathology: hepatitis and cholestatic. The pathogenetic mechanism of hepatitis is relative perivenular hypoxia caused by an increase in liver oxygen demand without an increase in hepatic blood flow. Progressive liver damage is possible in conditions of severe hypoxia. In case of cholestatic disorders, there is an increase in the level of alkaline phosphatase, gamma-glutamyl transpeptidase and bilirubin, indicating cholestasis.
Thus, in hypothyroidism, there is a violation of the bile-forming, bile-excretory functions of the liver, the formation of cholestatic syndrome. The liver is directly involved in regulating the metabolism of thyroid hormones, regulates their systemic endocrine effects, and can also act as a regulator of free thyroxine levels in the blood, changing the rate of excretion and reabsorption of hormones.
It is important to note that the liver synthesizes glucose transporter proteins (GLUT 1-5), among which GLUT 4 is the most important glucose transporter. Accordingly, the amount and activity of these proteins directly affects carbohydrate metabolism, and in case of liver dysfunction, this will affect the processes of carbohydrate metabolism.
Thus, liver dysfunction in hypothyroidism aggravates the disease and contributes to its progression and the formation of IR due to atherogenic dyslipidemia caused by a decrease in the synthesis of enzymatic regulators of lipid metabolism, due to frequent inflammatory changes in the hepatobiliary system, due to hypokinetic dysfunction of the biliary tract and cholestasis, which reduce the secretion of bile acids, important regulators of lipid metabolism, as well as due to a negative effect on the synthesis and activity of glucose transporter proteins (GLUT 1-5), which creates prerequisites for the occurrence of carbohydrate metabolism disorders.
Arterial hypertension and hypothyroidism. Contrary to the traditional belief that hypothyroidism is accompanied by hypotension, it has been established that in hypothyroidism, 15-28% of patients have hypertension, which is caused by an increase in total peripheral vascular resistance and arterial stiffness and is of low renin origin. The increase in peripheral vascular resistance is also due to compensatory hemodynamic mechanisms in response to low stroke and minute blood volume. It is believed that the severity of hypothyroidism correlates with the degree of increase in diastolic blood pressure, while systolic blood pressure increases to a lesser extent. An additional argument is the fact that replacement therapy in some patients with hypothyroidism leads to normalization of elevated diastolic blood pressure. Given the latest research, in particular the proven IR in hypothyroidism, hypertension can also be considered through sequential reactions caused by hyperinsulinemia. Insulin, acting directly on blood vessels, causes their dilatation. But in IR, the vasodilating effect of insulin disappears. Chronic hyperinsulinemia causes paradoxical vasoconstriction and an increase in the minute volume of blood flow as a result of stimulation of the sympathetic nervous system, an increase in the volume of circulating blood due to increased reabsorption of sodium and water ions in the proximal and distal tubules of the nephron, endothelial dysfunction, and finally, narrowing of the lumen of the arteries due to the proliferation of their smooth muscle cells. That is, chronic hyperinsulinemia leads to the development of hypertension. Some studies indicate the prevalence of nocturnal hypertension in patients with IR, which may be associated with a disturbance in the circadian rhythm of sympathetic activity under the influence of hyperinsulinemia and increased levels of FFAs in the blood plasma.
Thus, the analysis of literature data indicates insufficient study of metabolic disorders in MS in patients with changes in the functional state of the thyroid gland. Thus, MS is one of the most controversial syndromes. At the same time, despite the presence of a significant number of studies on the frequency and prevalence of MS in different regions, it should be emphasized that only a few studies have been conducted covering the population of different climatic and geographical zones and studying the functional state of the thyroid gland. The influence of impaired thyroid function on the realization of the insulin effect is currently being investigated in few studies. This indicates the relevance of studies on the diagnosis and treatment of MS in combination with thyroid disease, especially those associated with thyroid hypofunction. Thus, the need to improve the methods of diagnosis and treatment of patients with MS with type 2 diabetes is due to the fact that until recently, in the treatment of patients with this pathology, due attention was not paid to the functional state of the thyroid gland.
Results of personal research. On the basis of the Department of Endocrinology of Ivano-Frankivsk National Medical University, 360 people permanently residing in the Carpathian region of Ukraine were examined, including 330 patients with MS with type 2 diabetes and hypothyroidism who were inpatients in the endocrinology department of the regional clinical hospital.
The examined patients were divided into four groups depending on the presence of ID and hypothyroidism. As a result of the study it was proved:
- MS in conditions of iodine deficiency, in addition to the standard components of MS according to the IDF criteria, is characterized by a decrease in thyroid function, impaired humoral mechanisms, imbalance of adipocytokines, proinflammatory cytokines, TSH and cortisol hormones, formation of IR, persistent immunological abnormalities, disintegration of antioxidant defense, increased oxidative stress, formation of NAFLD, and increased risk of total cardiovascular mortality.
- The prerequisites for the development of hypothyroidism-induced MS in patients with type 2 diabetes mellitus under the conditions of YD are unsatisfactory glycemic control, the formation of high-grade IR, hyperinsulinemia and hypercortisolemia in the setting of hypothyroidism, which is confirmed by a direct correlation between IR (by HOMA IR) and TSH levels (r=0.5837, p=0.0001).
- MS with type 2 diabetes mellitus in combination with hypothyroidism is characterized by severe dyslipidemia, progression of IR, oxidative stress, and disintegration of antioxidant defense enzymes. The presence of a significantly higher degree of oxidative stress and deeper suppression of antioxidant systems in patients with MS with type 2 diabetes mellitus in combination with overt hypothyroidism has been shown. The correlation of dyslipidemia with TSH confirms the presence of cardiovascular risk in MS with type 2 diabetes mellitus in combination with hypothyroidism.
- An important role in the mechanism of IR belongs to the imbalance of serum enzyme activity. The peculiarity of patients with MS with type 2 diabetes mellitus in combination with hypothyroidism is a more significant increase in the activity of aspartate aminotransferase (AST) and alanine aminotransferase (ALT) and a decrease in the concentration of cholinesterase. A correlation between the functional state of the thyroid gland and the activity of liver enzymes has been proven.
- A characteristic feature of hypothyroidism-induced MS is an imbalance of adipose tissue hormones: a decrease in adiponectin (6.5 times) and an increase in resistin (2.3 times) in the blood serum. An inverse correlation was found between HOMA IR and adiponectin in all examined patients with MS (r= -0.3593, p=0.003). It was especially pronounced in the group of patients with MS with type 2 diabetes mellitus in combination with hypothyroidism (r= -0.8972, p=0.039), in patients living in a dietary facility (r= -0.5575, p=0.004), and in patients with non-alcoholic steatohepatitis (NASH) (r= -0.4698, p=0.004). The inverse correlation between TSH and adiponectin levels was found in all patients with MS (r= -0.2651, p=0.0418), and in the setting of YD (r= -0.4723, p=0.031) in patients with NASH (r= -0.5052, p=0.006). The serum adiponectin content also negatively correlated with the severity of dyslipidemia, abdominal obesity (AO), TNF-α and cortisol. An inverse correlation was found between HOMA IR and ioduria (r=0.238, p=0.0052).
- Hypothyroidism-induced MS with type 2 diabetes mellitus under conditions of iodine deficiency is characterized by the formation of microinflammation, activation of the proinflammatory cytokine system (4.2-fold increase in TNF-α, 6.9-fold increase in IL 6) and acute-phase proteins (11.8-fold increase in CRP) and plays an important role in the formation of IR syndrome. The interrelation of the power of the inflammatory response with the functional state of the thyroid gland and IR has been proved. A direct correlation was found between the level of TSH and TNF-α (r=0.692, p=0.001), TSH and IL 6 (r=0.584, p=0.001), TSH and CRP (r=0.549, p=0.001).
- Persistent immunological abnormalities were noted in patients with type 2 diabetes mellitus in the setting of YD, which we classify as secondary acquired non-AIDS-associated metabolic immunodeficiency. Two variants of immunopathological disorders have been identified: The first variant is a violation of the function of cellular immunity, phagocytosis with compensatory activation of the humoral immunity; the second variant is manifested by a decrease in the total number of T-lymphocytes (CD3) by 22%, helper T-lymphocytes (CD4) by 45%, T-cytotoxic lymphocytes (CD8) by 27%, a decrease in the immunoregulatory index (CD4\CD8) to 1.23, a decrease in IgG levels and an increase in IgM and IgA levels. It is prognostically unfavorable and is characteristic of hypothyroidism-induced MS with type 2 diabetes.
- Differentiated treatment of patients with hypothyroidism-induced MS with type 2 diabetes mellitus in the setting of diabetes mellitus using L-thyroxine and potassium iodide, hepatoprotectors, statins against the background of basic glucose-lowering therapy (metformin) allows normalizing thyroid function.
The present results of the study indicate a close relationship and interdependence of disorders of carbohydrate and lipid metabolism, oxidative stress and antioxidant defense, neurohumoral, immunological mechanisms of homeostasis, functional state of the liver and thyroid, adipose tissue hormones and adipocytokines in patients with type 2 diabetes mellitus in the conditions of diabetes mellitus. This allowed us to formulate a new general pathogenetic concept of the development and progression of hypothyroidism-induced MS in patients with type 2 diabetes mellitus living in conditions of iodine deficiency, taking into account the new data.
Hypothyroidism-induced MS is a group of clinical and metabolic disorders: abdominal obesity, hypertension, NAFLD, chronic hyperglycemia, poor glycemic control, hyperinsulinemia, hypercortisolemia, IR, dyslipidemia, oxidative stress, disintegration of antioxidant defense, adipocytokine imbalance – decreased adiponectin and increased resistin levels, activation of the proinflammatory cytokine system (IL 6, TNF-α) and acute-phase proteins against the background of reduced functional state of the thyroid gland (Fig. 1).

Figure 1. Pathogenetic concept of hypothyroidism-induced MS
Thus, the diagnosis of hypothyroidism-induced MS in patients with type 2 diabetes mellitus in the setting of iodine deficiency is based on generally accepted criteria. First of all, in the presence of abdominal obesity (waist circumference less than 80 cm in women and less than 94 cm in men; BMI more than 24 kg/m2), hypertension (blood pressure level more than 130/85 mm Hg ), dyslipidemia (blood cholesterol more than 4.8 mmol/l, blood LDL more than 3.0 mmol/l, blood HDL less than 1.03 mmol/l in men and 1.29 mmol/l in women, blood TG more than 1.7 mmol/l), IR, steatohepatitis, heart disease. The specific criteria for hypothyroidism-induced MS in patients with type 2 diabetes mellitus are the determination of serum levels of TSH, T3, T4. In the diagnosis of MS in the setting of iodine deficiency in patients with type 2 diabetes mellitus, we recommend establishing not only the presence of IR and hypothyroidism, but also their severity according to HOMA IR, respectively: HOMA IR = fasting blood glucose (mmol/L) × fasting blood insulin (μU/mL) / 22.5 (normal ≤2.77) and TSH level in the blood. Insulin resistance of the first degree should be considered at HOMA IR levels in the range of 2.78-19.0, the second degree – 20.0-50.0, and the third degree – >50.0.
The risk factors for hypothyroidism-induced MS are mature and elderly age, overweight, type 2 diabetes mellitus, dyslipidemia, increased ALT activity, ALT/ALT more than 1, activation of oxidative stress and suppression of antioxidant systems, decreased adiponectin levels and increased serum resistin levels, hyperactivation of certain proinflammatory cytokines (IL 6, TNF-α) and acute-phase proteins (elevated CRP levels), depletion of the cellular immune system (decreased levels of CD3, CD8, CD16, CD4\CD8), suppression of humoral immunity (insufficient IgG levels), overt or subclinical hypothyroidism. We have proposed an algorithm for the diagnosis of hypothyroidism-induced MS (Fig. 2).
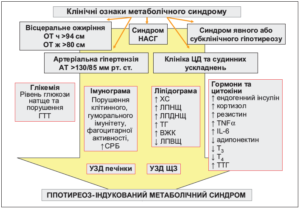
Fig. 2. Algorithm for the diagnosis of hypothyroidism-induced MS
The main idea behind the concept of hypothyroidism-induced MS is to identify a population at high cardiovascular risk. Therefore, preventive measures to modify lifestyle and use of adequate medications can significantly improve health indicators and prevent the onset and progression of both atherosclerotic vascular disease and type 2 diabetes, which, in turn, are inextricably linked to increased morbidity and mortality in the population.
Thus, the need to improve the methods of diagnosis and treatment of patients with MS with type 2 diabetes is due to the fact that until recently, in the treatment of patients with this pathology, due attention was not paid to the functional state of the thyroid gland, the degree of IR, the phenomena of steatosis and steatohepatitis, and immunological abnormalities. In this regard, there is a problem of in-depth study of the mechanisms of therapeutic effect and therapeutic efficacy of new drugs correcting disorders of the metabolic link of homeostasis, IR, immune system, and functional state of the thyroid gland in the setting of ID.
We have proved the effectiveness of the use of metformin, a biguanide drug, in type 2 diabetes mellitus in combination with hypothyroidism. The effectiveness of the use of lipid-lowering drugs (statins), which are effective means of pathogenetic therapy of patients with type 2 diabetes mellitus and hypothyroidism in order to normalize the lipid spectrum of the blood, has been established. Prescribing potassium iodide is the most appropriate method of treating endemic goiter.
Thus, it is recommended to supplement the algorithm for the diagnosis of MS according to the IDF criteria in the setting of iodine deficiency by determining the function of the thyroid gland by the level of its hormones in the blood serum (TSH, free T3 and T4), ultrasound of the thyroid gland, it is necessary to establish the presence of IR, hypothyroidism, their severity by HOMA IR: HOMA IR = fasting blood glucose (mmol/l) × fasting blood insulin (μU/mL) / 22.5 (normal ≤2.77), which makes it possible to increase the effectiveness of early diagnosis and treatment of hypothyroidism and prevent cardiovascular complications.
In order to predict the development of hypothyroidism-induced MS, it is recommended to determine its risk factors: mature and elderly age of the patient, overweight, type 2 diabetes mellitus, dyslipidemia, increased ALT activity, ALT/AT ratio >1, activation of oxidative stress and suppression of antioxidant systems, decreased adiponectin levels and increased serum resistin levels hyperactivation of proinflammatory cytokines (IL 6, TNF-α) and acute-phase proteins (elevated CRP levels), depletion of the cellular immune system (decreased levels of CD3, CD8, CD16, CD4\CD8), suppression of humoral immunity (insufficient IgG levels), overt or subclinical hypothyroidism.
In the setting of iodine deficiency in the presence of MS, it is recommended to determine the median ioduria and TSH level and prescribe potassium iodide at a dose of 200 mcg/day and, if necessary, L-thyroxine at a dose of 50-200 mcg/day. In the domestic pharmaceutical market, potassium iodide is represented by Yodofol (potassium iodide 200 mcg and folic acid 400 mcg) by World Medicine. In order to normalize blood lipid spectrum in patients with type 2 diabetes mellitus with iodine deficiency, it is recommended to use lipid-lowering drugs.
In patients with type 2 diabetes mellitus with NAFLD, it is recommended to include hepatoprotectors in the treatment complex. This helps to eliminate clinical and biochemical signs of steatohepatitis, insulin resistance, normalize glycemia and insulinemia, improve liver function, blood lipid balance, and slow the progression of steatohepatitis.
The priority of the results of our research is also confirmed by two declarative patents of Ukraine for utility model (Pat. 41756U, MPC (2009) A61K31/35. Method of immunocorrection in patients with type 2 diabetes mellitus with metabolic syndrome / N.V. Skrypnyk, I.O. Yakubovska (UA) applicant and patentee N.V. Skrypnyk, I.O. Yakubovska (UA) – № u200814162; application for application for a patent for Ukraine (08.12.2008; published on 10.06.2009, Bulletin № 11. – 6 p.; Pat. 43857U, MPC (2009) A61V5/00. Method for diagnostics of hypothyroidism-induced metabolic syndrome / N.V. Skrypnyk, P.M. Bodnar (UA) applicant and patentee N.V. Skrypnyk, P.M. Bodnar (UA) – № u200814323; application for a patent filed on 12.12.2008; published on 10.09.2009, Bulletin № 17. – 6 p.). In addition, we have developed 2 innovations, which are included in the Sectoral Register of Innovations.